I have been interested in autism for about 30 years thanks to my son Oscar. Children can lead you in interesting directions.
My cute little boy walked on his toes, flapped his hands, was not interested in playing with other children, liked to spin the wheels of his toy for hours, screamed inside the supermarket, and when he eventually started to talk referred to himself in the third person. He soon knew everything there was to know about aircraft and airlines.
I was lucky – in those days agencies worked together and even though he didn’t yet have the label of autism he had a great team of professionals who put him in the centre, at home and at playcentre. I was also lucky to have a supportive family and community.
When you have a child who is different your instincts are often to ask why, find out what is it you are dealing with and what can be done. With autism the first two raise too many unknowns and most parents I suspect just get on with getting on. Which for autism usually means a lot of advocating. For me it also meant researching until I got a PhD in 2011 on autism policy, in trying to understand why it all seems so hard to get right. I was lucky to get research funding from the Health Research Council.
I looked at the history of autism and of the disability rights movement and tested some public policy theories, and talked to a lot of people, family members, policy and support people and people on the spectrum.
I found that autism is so complex that it could be considered a ‘wicked’ problem (more about that later). But also that good outcomes for a person on the spectrum largely depend on love and luck, as suggested by my friend Matt Frost, which in practice means having the love of someone (often a mother) who will advocate for you and your needs forever if necessary, and the luck to find the right people and services when you need them. Love and luck depend on chance, so are not a good basis for public policy.
So what is autism?
Everyone probably has their own idea. Perhaps it is a person or people you know, a family member, or maybe you identify as a person on the spectrum. There is a huge variety in how autism presents and what it looks like. As the saying goes if you’ve met one person with autism, you have met one person with autism.
When I first got interested in the topic in the 1990s the concept of autism was dominated by the 1988 movie Rain Man. The character with autism played by Dustin Hoffman was loosely based on Kim Peek, an autistic savant, and was also influenced by Oliver Sacks’ writings. With the addition of a great deal of artistic license. So an autistic man was shuffly, lived in an institution, had savant abilities and frustrated his cool brother who was played in that movie by a young Tom Cruise. Rain Man dominated ‘what autism is’ for years.
Yet there were several other portrayals of autism in movies of the era including Peter Sellers’ Being There and a very youthful Leonardo di Caprio in What’s Eating Gilbert Grape ‒ although autism is not mentioned in either of those movies.
Autism can be a code for a type of behaviour that is different, sometimes scary or confusing. And the code and the label changes over time. And the label itself is contested. Which is all problematic for public policy.
When I first learned about autism in the 1990s I heard about the ‘triad of impairments’ which was the language of the time from the diagnostic bible the US Psychiatric Association’s Diagnostic and Statistical Manual (DSM). The triad involved problems – it was framed in negative clinical language ‒ with social interaction (mind blindness), communication (non or unusual use of language), and restricted interests and activities.
Not surprisingly, as these criteria were developed from the observations of clinical outsiders, there was no recognition of the sensory sensitivities of hearing, vision, touch, taste and smell which we now know are a critical aspects of autism. Clinicians saw tantrums rather than meltdowns caused by sensory overload (which can be manifested for example by the child putting their hands over their ears or in limited food preferences).
Today we know that these sensory sensitivities, and the so-called triad of impairments can also be positive. Many autistic people credit their particular autistic gifts for artistic, engineering, IT or other achievements. As autistic animal behaviourist and writer Temple Grandin has said, probably the major inventions in the world came from people with autism because the rest were too busy socialising.
Where has autism come from?
I suspect there have always been people with autism – in every culture. But with the rise of the science of psychology and psychiatry in the early 20th century it was inevitable that autism would be studied and named. The ‘aloneness’ (autos ‒ Greek, autismus ‒ Latin, meaning self) of certain children fascinated many and the idea of autism was used about 100 years ago by a Swiss psychiatrist, Eugen Bleuler, to describe a type of schizophrenia. Ominously, he also advocated the sterilisation of people with schizophrenia. Soon the Nazi era would influence significant developments in autism.
Many of the academics and leading clinicians in Germany and Austria were Jewish and they started leaving Europe in the 1920s to escape growing anti- Semitism and discrimination. One of those who left was Austrian Leo Kanner.
Kanner was born in the 1890s in what is now part of Ukraine and studied at the University of Berlin. He immigrated to the US in the 1920s and eventually became the America's first specialist child psychiatrist. He was based at Johns Hopkins Hospital in Baltimore. But he did not work alone. As he became established in the US he encouraged and sponsored many of his Jewish colleagues to leave Europe and join him in his developing work on autism. One who did was Georg Frankl, who had been working as a diagnostician with Hans Asperger in Vienna in the 1930s before being employed by Kanner in 1937.
In 1943 Kanner published a significant paper ‘Autistic disturbances of affective contact’ about a group of children he had been studying. He described a condition which he called early infantile autism that could have been caused by poor parenting (meaning distant or cool parents). So Kanner was establishing a diagnostic culture for autism. He published an influential text book called Child Psychiatry which was republished several times over the decades.
Meanwhile in Vienna, a young Austrian paediatrician named Hans Asperger was working at the University Children’s Hospital in Vienna. The first killings by the Nazis started after a German father asked the state’s doctors to euthanise his disabled son. That was the beginning of the mass killings – starting with disabled children and extending to adults and then to other groups, including Jews.
I like to think that as a paediatrician working under the Nazi regime Asperger described the children he was working with as ‘little professors’ to save them. He also suggested autism was a spectrum and supported education for autistic children. This history is contested (and Wikipedia is currently very anti Asperger) but for details of this fascinating era I recommend Steve Silbermans’ recent book Neurotribes.
Asperger’s autism thesis of 1944 did not reach the English speaking world English for several decades until it was translated and championed by UK autism experts Lorna Wing and Uta Frith in the 1980s, after Asperger’s death. For a while Kanner's Autism described those with high and complex needs and Aspergers the so-called high-functioning end of the spectrum. But it appears that the two groups of children studied were very similar.
A few years ago journalists tracked down Kanner’s child no 1, Donald Triplett, and found he lived an independent life in his 70s, including driving himself to golf. His life provides a salutory lesson in not taking an initial diagnosis too negatively.
Meanwhile the blaming of parents for this strange condition persisted. Into the picture came another Jewish American, Bruno Bettleheim. He had been briefly imprisoned in a concentration camp in 1938, released in 1939 and went to the US where he became an apparently self-taught professor of Psychology at the University of Chicago. He was also an early proponent of pop psychology and his 1967 book The empty fortress remained influential for decades. He popularised the term ‘refrigerator mothers', those cold and emotionally detached parents who were the cause of their child’s autism, which he likened to being in a concentration camp but caused by maternal deprivation. In New Zealand this theory made it very difficult for the parents of the few children with diagnosed autism to set up support groups and fundraise.
Autism in New Zealand
In New Zealand in the 1950s and 1960s there were high levels of institutionalisation of disabled children, including those who today would be diagnosed with autism. Eugenics-based public policy had for decades advocated that disabled children should be locked away and families should forget about them. Hundreds of disabled children, young people and adults lived in institutions such as Kimberley near Levin.
But some mothers wanted a better life for their children. One was Marion Bruce who died earlier this year and who helped me a lot with my research. She recalls that her youngest son was ‘different’. In the 1960s she tried to find a local school to take him and community support, without success.
Retired British child psychiatrist Mildred Creak visited New Zealand at that time as she had Quaker relatives in Wanganui. Mildred Creak is another of the significant people in autism history – an age contemporary of Hans Asperger born around the turn of the century.
Creak diagnosed young Andrew Bruce and a few other New Zealand children using the specialised diagnostic tool she had developed. She encouraged Marion to get together with other parents for support and to find out more about this puzzling condition. So in 1967 Marion and her husband went to Adelaide in Australia for the first autism conference in the southern hemisphere. She gave me a copy of the proceedings. It was progressive for the time (remember this was the same year as Bettelheim’s book) and mainly considered the educational potential of autistic children.
A keynote speaker was a young child psychiatrist from London called Dr Michael Rutter, another Quaker. In his presentation he called ‘infantile autism’ a rare disorder occurring in about 3 or 4 children out of every 10,000, three or four times as frequent in boys as in girls with a tendency for autistic children to come from the middle class. The condition usually manifested by the age of two and a half.
Rutter critiqued the operant conditioning of behaviourist psychologist Skinner which was then being publicised by Lovaas and is the basis of today’s ABA therapy. He called on adults to provide role models. He cited Kanner’s classic text Child Psychiatry, but challenged Kanner in overlooking the educational potential of such children and his talk was about the principles upon which the education of autistic children should be based. That marked a significant change in direction.
Today, in his 80s, Dr Rutter is an influential and still practising child psychiatrist – and also an advisor to the Dunedin Longitudinal Study. He learned from Kanner, but his more positive approach to children with autism and their families has been influential.
Every country has its own autism history but the circle of international influencers is quite small and our history shows that New Zealanders were up with the latest theories.
However, at that time the only place which would provide any educational support for Marion’s son was Hohepa and he remains in their care today. Marion helped develop a parents’ autism support group in 1969, initially under the umbrella of the Intellectually Handicapped Children’s Assn (later the IHC). Thirty years later the organisation become Autism NZ. Marion joined the Wellington Hospital Board and managed to establish Puketiro as a diagnostic and respite centre. She told me about the relief that followed research showing autism was genetic and not caused by bad parenting, as that stigma had made life difficult for parents for many decades.
The Disability Rights movement
Meanwhile in New Zealand and worldwide the disability rights movement was gaining momentum
A few milestones in NZ:
1975 The Disabled Persons Community Welfare Act provided the first disability allowance, respite and carer support
1980s Rise of the self-advocacy People First movement
1989 Education Act legislated for the right of all children to go to their local school from 5-19 years
1993 Human rights Act included disability as grounds
1999 First Minster of Disability Issues soon followed by the establishment of the Office for Disability Issues
2001 The NZ Disability Strategy recognised the social model of disability – that people have impairments but society creates disability and can also address those disabling environments and policies
2006 The last psychopaedic institution, Kimberley, closed
2008 Ratification of the UN Convention on the Rights of Persons with Disabilities.
There were also some significant policy changes affecting autism.
In 1993, disability support went from the Department of Social Welfare to the Ministry of Health. People now sought support through a gatekeeping Needs Assessment and Support Coordination (NASC) system with narrow eligibility criteria of only intellectual, physical, hearing or vision impairment.
The 1994 DSM IV contained the diagnosis of Aspergers syndrome ‒ autism without intellectual disability ‒ for the first time, but it would be 20 more years until people with autism and without ID could access NASC.
In 1996 the new policy of Special Education 2000 brought in targeted ORS funding for only 1% of children and a small Special Education Grant for each school. There have been several major reviews since, which have all highlighted the lack of support for autistic students.
In 1997 a mother killed her autistic teenage daughter which resulted in two major inquiries, known as the Curry Report (internal to the Ministry of Health) and the official government response, the Werry Report. In the latter, significantly, Professor John Werry urged professionals to listen to mothers when they say their child is different, as they are usually right and need support.
Ten years of policy work on autism led to the 2008 NZ ASD Guideline, led by another autism champion, the late Joanna Curzon. For a few years there was a little bit of money for implementation but in 2016 most research in the Guideline is now 10 years out of date. For a fast moving field like autism that is significant. Last month some specific updates to recommendations were published.
So where are we today with autism?
We now have a new DSM 5th edition which describes one large autistic spectrum. Although it is US-based, the DSM influences much of the autism research and literature and diagnostic tools in the English speaking world and is similar to the guidance given by the World Health Organisation’s International Classification of Disability.
Prevalence
Just as diagnostic data is fluid and contextual, so are the estimated numbers of people with autism. Thirty years ago it was considered a rare condition affecting perhaps 2-3 children in 10,000 people. Then Aspergers entered the DSM VI in 1994 and by the early 2000s it was 1 in 100. By 2012 the number had jumped in the US to 1 in 88 and by 2014 the US Centers for Disease Control and Prevention, the government agency responsible for such data, estimated that 1 in 68 children had an autism spectrum disorder.
This new estimate was based on data from 8-year-olds across the US, ranging from 1 in 175 children in Alabama to 1 in 45 children in New Jersey. Researchers reviewed records from community sources that educate, diagnose, treat and/or provide services to children with developmental disabilities.
The data showed that ASD was almost five times more common among boys than girls: 1 in 42 boys versus 1 in 189 girls. White children were more likely to be identified as having ASD than black or Hispanic children. Levels of intellectual ability vary greatly among children with autism, with about half average or above average intellectual ability (an IQ above 85) compared to a third of children a decade ago.
But why this dramatic growth in numbers over the years – was something causing an epidemic?
Earlier this year, new autism statistics from the Center for Disease Control and Prevention suggested that autism is steady at the same 1 in 68 prevalence in schoolkids across the country as two years previously. This was the first time since 2002 that the agency released new autism numbers that did not reflect an upward trend.
Autism remains more commonly identified among white children as compared to non-white kids. And the condition is far more prevalent among boys.
What does all this indicate? I suspect it shows that diagnosis and services are more likely to go to white kids. Girls are probably underrepresented – perhaps the right diagnostic tools are not being used. And what about the adults?
But on the positive side, was can say that the whole scare debate of the last couple of decades about an autism epidemic has probably been due to increasing access to diagnosis and widening diagnostic criteria, rather than anything more sinister.
Today’s NZ data
We have little New Zealand data. Although the last census has a disability prevalence of 24% of people with a significant impairment lasting longer than 6 months, it does not have a specific category of autism and the Ministry of Education doesn’t use diagnosis labels.
However, the Ministry of Health’s NASC data from 2014, the first year autism in its own right became a criterion for NASC assessment, has recently been released. It shows 16% or 5077 people had autism as their primary disability (so a lot of people had been missing out on support). Many of those with ID, which was by far the largest group, also had ASD.
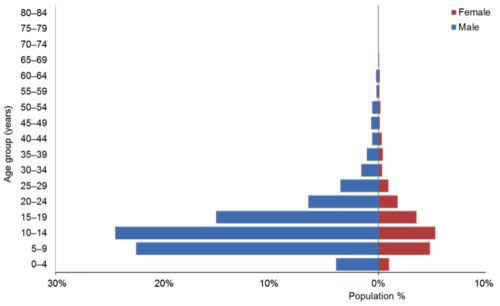
Figure 40: Age and sex of Clients with ASD
- The median age of clients with ASD is 12 years.
- ASD clients are predominantly male (81%).
- ASD clients are predominantly young (80% of ASD clients are aged under 20).
Carer support is by far the most common service usage.
So, a good start and we will be watching the trends from now on.
Minds for Minds is a clinical research group based at the University of Auckland which is crowdsourcing autism data from New Zealanders. The latest Minds for Minds newsletter (Issue #5, May 2016) reveals some new data:
Some of the key points to come out of this analysis are listed below:
• We observe the well-reported male to female gender bias (4:1)
• The population distribution reflects New Zealand’s latest census
• Anxiety disorders, depression and epilepsy were highly prevalent amongst individuals with ASD and their families
• 48.5% reported at least one other co-occurring condition The most common co-occurring condition in those under 7 is ADHD, then in decreasing frequency dyspraxia, followed by depression and anxiety
The most common condition in those aged 8 to 17 was depression and anxiety, then in decreasing frequency ADHD, followed by dyspraxia
The most common condition in those over the age of 18 was depression and anxiety, then in decreasing frequency gastrointestinal symptoms, followed by ADHD
• The number of co-occurring conditions increased with age
• 91.2% of individuals reported one or more condition among first-degree relatives
• The most common conditions occurring in relatives were ADHD, depression and anxiety, ASD
They are also doing genetic testing of volunteers and ‘observing just how varied and complex the genetics of ASD can be’… ‘involving several different regions of a person’s DNA including multiple chromosomes’.
Yet despite all this progress we still have people with autism institutionalised, sometimes in seclusion. One is Ashley Peacock, a victim of an abusive and uncaring system. Despite the best efforts of his parents over many years, and some prominent media coverage, he remains institutionalised under the mental health system.
And as for the numbers of people with autism locked up in our justice system – we have no idea.
Meanwhile, people with autism have an estimated life expectancy of about 20 years less than those without.
So what about autistic adults? It is an unresearched area. There is not even a straightforward diagnostic pathway for autistic adults in our public health system.
Competing autism agendas
Autism is not something that can be seen, touched or measured. There are different and often conflicting agendas. So how to make sense of it?
An attempt at sorting the competing agendas has been made by US academic Dana Lee Baker (2011). She writes about cause, cure, care and celebration.
Cause attracts the bulk of research money and status.
Although not evidence-based, seeking a cure for autism is big business – and some parents use dangerous interventions such as testosterone injections for their children, or dosing with bleach.
Care sees autism as a negative economic cost.
Celebration of autistic identity and neurodiversity is the preferred approach for self-advocates and some families.
I like to think that celebration of the diversity of humanity could also underpin an inclusive future which also values caring and nurturing.
Meanwhile, most weeks there is the latest theory about the causes of autism – with many confusing causation and correlation. But latest research indicates a complex interaction between genes and environment, a condition which is highly heritable, to do with brain connections and possibly gut microbiome. For me though, it is more important that everyone belongs in an inclusive community which is welcoming of diversity.
So drawing all these threads together it seems obvious to me that we are dealing with a ‘wicked’ policy problem. A ‘wicked’ problem is resistant to an easy solution with no one definition of the problem, is socially complex and risks unintended consequences with any interventions.
The only way forward is to be innovative, so we could start by giving policy power to people with autism and their families and allies. Perhaps we could let the self-advocacy movement find their own solutions for their own lives, deal with their own conflicts and create their own leaders?
How about the future?
Technology will continue to have a huge influence. Those apparently non-verbal autistic people, can now ‘talk’ through technology such as iPads and smart phones and can tell us a lot. Of course, they also need access to the technology and particularly the skilled teaching in how to use it. I urge people to presume competence in anyone with a diagnosis of autism, however impaired they appear, as they probably know and understand a lot more than the rest of us assume.
As well, we neurotypicals (those of us without autism) need to find more effective ways of talking and communication with people with autism – we should perhaps take care to be more literal and logical and use fewer metaphors and colloquialisms and keep instructions simple.
What I have observed is that there is often a lot of anxiety in people with autism and it is largely caused by not being able to predict the future. Just because something happened yesterday does not mean it will happen today. We need to be sensitive to that anxiety and explain carefully the full sequence of what will happen in daily activities and what needs to be organised to ensure it all goes smoothly.
I have noticed a great deal more awareness of autism in the last 20 years or so, which is not surprising if prevalence is 1 in 68. That means each school and community has people with autism and their families.
Employment is a big issue for many. We need patient and flexible employers who see strengths not weaknesses. Our welfare system is punitive and keeps many in poverty. So a Universal Basic Income could remove a lot of anxiety and stress and value the various way autistic people contribute to society.
I would like more integrated support systems around the person with autism.
I would like to see people with autism find their place in an inclusive society and not have to depend on having the love of a family and the luck to find good supports.
Parents are important. Parents can be the key to their children’s inclusion After all my research I realise firstly and forever I will be a parent of child with autism. As parents of children, young people and adults with autism we all probably accept that this job is for a life time. The future is always a worry.
So there are many threads in the autism story.
It is a Māori perspective on time and progress that we walk backwards into the present and future. So we acknowledge and bring the work and wisdom of those who have come before with us in our work and understanding of the present situation and in anticipating the future.
Walking backwards into the present and into the future and seeing where we have been, and acknowledging those who went before, highlights the complexities of a fascinating condition that is hard to describe or pin down.
Personally, I hope there will still be people with autism in the future and I hope they are valued.
But there is never a last word on autism.
–––
(Edited from a presentation at Victoria University, 13 July)