This week, Helen Kelly, who has metastatic lung cancer and is terminally ill, received a letter from the Ministry of Health to tell her that an application by her oncologist Anthony Falkov under Sections 20-22 of the Medicines Act to import and prescribe cannabis oil inhalers to treat nausea, anorexia and pain has been "deferred".
Specifically:
The Ministry assessed Dr Falkov's application and considered it to contain insufficient information to enable a decision to be reached, briefing Associate Minister of Health Hon Peter Dunne accordingly.
Consequently, a ministerial decision was made on January 29 to defer the application.
Mr Dunne directed the ministry to follow up with Dr Falkov to obtain the oustanding information to allow an informed decision to be reached.
The ministry's response was swift: it was made the day after Dr Falkov's application was application was received. Subsequent delays appear to have been a matter of difficulty in contacting Dr Falkov. The response was also disingenuous and somewhat inevitable.
The "outstanding information" supposedly being sought from Dr Falkov is information that would help the application meet all the criteria used to guide the process of ministerial approval to import and use non-pharmaceutical-grade medical cannabis products.
These criteria are not stipulated in the Medicines Act. They were drawn up only relatively recently, in response to the Alex Renton case. I have an outstanding Official Information Act request as to how the criteria were prepared and on what advice. In my non-expert view, the criteria are unreasonable and, in this case, not fit for purpose.
Helen has sent me photographs of the three pages of the ministry's response and I've uploaded those in the first comment for this post. But it's worth going through them:
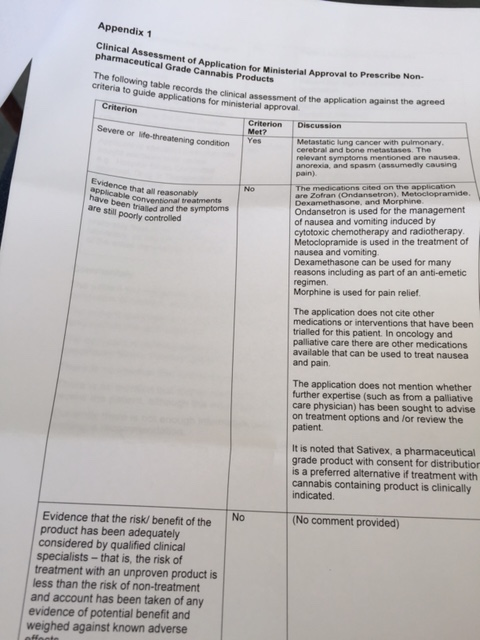
a. severe or life-threatening condition
Yes. Helen has metastatic lung cancer which has spread to her bones and her brain.
b. evidence that all reasonably applicable conventional treatments have been trialled and the symptoms are still poorly controlled
No. Helen is taking morphine for pain and three different drugs to try and manage nausea. But according to the ministry, "The application does not cite other medications or interventions that have been trialled for this patient." Now, remember that Helen has already taken a cannabis preparation and says that helped her sleep and manage her pain in a way that morphine doesn't. But under the criteria, that is immaterial unless the doctor can literally show that everything else has been tried.
The response also faults Dr Falkov for failing to seek advice from a palliative care specialist. It will be interesting to discover whether and to what extent the ministry has itself done this in devising the criteria, which themselves make no specific reference to palliative care.
The response also cites Sativex as "a preferred alternative if treatment with cannabis containing product is indicated". But Sativex is a pharmaceutical grade product – it's approved for use in New Zealand, but not funded. This is an application to use a non-pharmaceutical-grade product, under the rules for such an application. The ministry's response is disingenuous and irrelevant. Moreover, Helen says Sativex is unlikely to manage her symptoms as well.
c. evidence that the risk/ benefit of the product has been adequately considered by qualified clinical specialists – that is, the risk of treatment with an unproven product is less than the risk of non-treatment and account has been taken of any evidence of potential benefit and weighed against known adverse effects
No. The ministry has declined to offer any comment on this section, so it's hard to know what evidence would be satisfactory. But Helen Kelly is dying. She has already taken a cannabis preparation. It's hard to see what further "risk of treatment" might be added by her taking a commercially prepared substitute. Or, indeed, who the "qualified clinical specialists" might be, beyond the senior oncologist treating her.
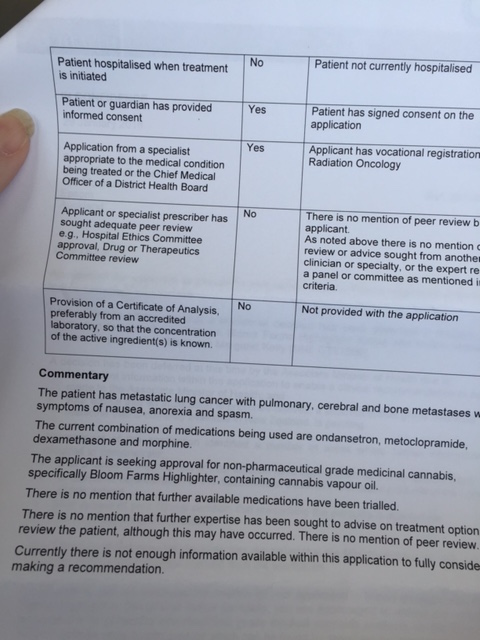
d. patient hospitalised when treatment is initiated
No. And this is another example of how these criteria are unreasonable and poorly designed for palliative care.
e. patient or guardian has provided informed consent
Yes.
f. application from a specialist appropriate to the medical condition being treated or the Chief Medical Officer of a District Health Board
Yes.
g. applicant or specialist prescriber has sought adequate peer review eg, Hospital Ethics Committee approval, Drug or Therapeutics Committee review
No. "There is no mention of peer review by the applicant. As noted above there is no mention of review or advice sought from another clinician or specialty or the expert [obscured] a panel or commitee as mentioned in the criteria."
I think Dr Falkov's application would have been well-served by a supporting statement from a medical ethics committee or similar. But by the same token, these are criteria drawn up for the specific purpose of guiding approval for non-pharmaceutical cannabis products. It would be nice to see some evidence the ministry itself had sought ethical advice in drawing them up. This is, after all, a kind of application that is likely to be repeated in form. It seems a high bar to require every specialist doctor to seek this kind of peer review to help a terminally ill patient.
h. provision of a Certificate of Analysis, preferably from an accredited laboratory, so that the concentration of the active ingredient(s) is known
Bloom Farms, which makes the products Helen wants to import, supplies "medical cannabis dispensaries" throughout California – but California's medical cannabis laws are very loose and Bloom Farms isn't really a pharmaceutical manufacturer. Its website repeatedly cites "our mantra: relaxation, relief, creativity and fun" but I couldn't find any formal statement of assay on its website beyond an assurance that its "pure, all-natural cannabis oil contains consistent 45-50% THC content."
It's not unreasonable to seek evidence that a medical product is what it says on the label. It might be unreasonable to demand that every doctor or patient pays for an individual lab analysis.
But another California company, Phytologie, does provide a medical cannabis quality asurance programme that it provides "to our members to share with their physicians, so that their doctors can assist with designing more precise strategies for using cannabis medicinally." Here's one assay of a Bloom Farms product conducted with Phytologie as the client. And another of a high-CBD product. So this kind of testing is done and presumably Bloom Farms would be able to provide this information on request.
In this last respect, I think it can fairly be said that Dr Falkov has failed to provide sufficient evidence for his application. An assurance of the purity and potency of a medicine is an entirely reasonable requirement. But he's an individual oncologist and presumably a busy one. Does the ministry have a plan to build a product register? Or set up a structure to help ensure the robustness applications under this part of the law? Wouldn't that save wasted time and unnecessary suffering?
This issue isn't going to go away and I think the ministry needs to do a much better job than is suggested by these swiftly-drafted criteria, which look in some respects as if they're designed to make the problem go away.
In particular, there should be some better thinking around palliative care. It doesn't make sense to treat every application to improve the quality of life of a dying person the same as a bid to give a sick child an experimental treatment. The criteria are ostensibly specifically dedicated to cannabis products, but they're actually entirely general. We need this to be done better and more transparently.
As I've noted before, the use of cannabis in palliative care represents a particular ethical case. If a patient testifies that the treatment does in fact improve their quality of life and ease suffering in a way that approved pharmaceutical products have not, that should count for a great deal. The case for preventing access becomes much, much harder to make.
Peter Dunne has previously said to me that the criteria are only guidelines and don't determine his ministerial decision. But he's a minister who likes to emphasise that he acts on expert advice. And perhaps he has no choice, given his limited stock of political capital in this area.
This is, after all, a government that has chosen to brand itself on never changing the law – either the Misuse of Drugs Act or the Medicines Act – no matter what the evidence. That was, remember Justice Minister Simon Power's response to the Law Commission's view that there was "no reason why cannabis should not be able to be used for medicinal purposes in limited circumstances" by declaring "There is not a single solitary chance that as long as I'm the Minister of Justice that we'll be relaxing drug laws in New Zealand."
Power is no longer Ministry of Justice, but every single initiative to improve the way we deal with drugs in New Zealand still has to climb around this entirely political edict. It's the key reason we have little prospect of dealing sensibly with a fast-changing environment.
During the last election campaign, Prime Minister John Key paid visits to several Kapiti Coast and Porirua schools. When he wasn't insisting that his favourite music was One Direction, Key fielded this question from a student at Kapiti College:
Asked whether he would legalise medical marijuana, he told the school assembly: "This is the fundamental message. Drugs are bad for you."
Yes, the Prime Minister really did say "Drugs are bad, m'kay?"
I sometimes find myself in the position of defending minister Dunne. And it's not that I don't believe he should be doing better – I think he should be – but because what's happening here is not so satisfyingly simple as a prohibitionist minister crushing all bids.
The good part is that the criteria for applications like Helen's can be improved without changing the law. They're not part of the Medicines Act. I think Peter Dunne needs to ensure, as minister, that the process is fundamentally improved. Because a process so designed as to frustrate all medical cannabis applications will not prevent the use of cannabis in this way.
In the end, we do need to revisit the law – as the Law Commisison and two Parliamentary select committee inquries have already said. Palliative care is not the only element of medical cannabis policy. But it's certainly the place we should start, given the growing use of cannabis this way in defiance of the law. When we fail to do this, we impose risk and stress on desperately ill people and their doctors – and we're saying we don't care enough to properly regulate for their safety.
No one is going to prosecute Helen Kelly for treating her symptoms with cannabis. But what the system currently says is that it can't and won't make that safer for her. We need to do better than this. A lot better.