As you might have noticed, there is considerable activity in the area of drug policy. It's only a week and half until the United Nations' top policy-making body, the General Assembly, meets to discuss just that topic.
Ironically, the two things that happened yesterday – Labour MP Damien O'Connor's private member's bill aiming to to ease access to medical cannabis and a new and revamped New Zealand Drug Harm Index – have no particular connection to UNGASS. The former aims to address the shortcomings in our current medical cannabis approval system highlighted by Helen Kelly's case, and the latter fulfils an undertaking in last year's National Drug Policy.
Although O'Connor's is a private member's bill, he has had access to resources in the leaders office in preparing it, and it has been signed off by the Labour caucus. O'Connor's bill emerged from the Alex Renton case and the MP described it at the time as an attempt to improve access to cannabidiol (CBD), the hemp-derived cannabinoid that Renton's doctors were eventually granted approval to use in treating the young man's persistent seizures. Until fairly recently, the party was telling journalists the same thing: that the bill aimed to improve access to CBD.
In that sense, there's a symmetry with the controversial criteria for ministerial approval of medical cannabis products. Those too were drawn up in response to response to the Renton case – in which CBD was seen as a last-chance treatment for an intractable medical condition. As Helen Kelly's application demonstrated, those criteria were barely fit for purpose with respect to the use that Kelly and pssibly thousands of others seek: providing relief from the symptoms of terminal illness and chronic pain.
The difference is that O'Connor's bill has evolved, while the criteria are still pending review.
What the Misuse of Drugs (Medicinal Cannabis Approval) Amendment Bill actually does is well summed-up in its explanatory note:
This Bill proposes to make it easier for patients with a terminal illness or who are suffering from a condition that gives them significant pain to be able to access a cannabis preparation product approval through the Ministry of Health.
It inserts a new section 8A in the Misuse of Drugs Act so that in exercising regulatory powers regarding the medicinal use of cannabis preparations in individual cases, the Minister must not prevent the supply and administration of cannabis preparations to a person considered by an appropriate vocationally registered practitioner to be in the final stages of a terminal illness or to have a permanent condition that causes a significant level of impairment or pain.
So the minister must approve the use of medical cannabis by any patient deemed to be suffering a terminal illness or "permanent", "significant" impairment or pain. This would have a particular effect. Rather than rejecting an unacceptable product (which is what happened, to some extent, in Kelly's case), the ministry would need to nominate acceptable products.
Actually, more than that. A Q&A sent out with the text of the bill says: "We would expect the Ministry of Health to be responsible for accessing suitable products."
I've said before that the ministry could draw up a register of approved products to avoid applicants wasting their time. But actual sourcing and supply is probably better. It's certainly better than leaving patients to fend for themselves. (This could of course be done without amending the Misuse of Drugs Act, but only by the government. Labour can't instruct ministry officials from Opposition.)
Peter Dunne has already said that work in Australia is likely to lead to a wider range of approved medical cannabis products both there and in New Zealand. The bill, should it be drawn from the ballot and passed would bring forward that day via products from, say, Europe and Israel.
So in that sense it's not really hostile to the path Dunne has already laid out. It's also quite amenable to further work at select committee, where questions on standards and potency could be addressed. It could be seen to privilege pain and palliative care over therapeutic use of CBD, but that, too, could be considered by a select committee.
The Q&A offers a blunt "no" in answer to the question of whether Labour is even considering cannabis decriminalisation – which actually makes Dunne the liberal on that issue – but Labour has identified a real problem and proposed a relatively straightforward means of addressing it. This isn't bad.
–––
Back in 2008, I examined the new New Zealand Drug Harm Index and wrote a damning blog post about it it headed Spectacular but useless. The whole thing was essentially an expensive PR exercise for the police, with a flimsy connection to social science and almost nothing in the way of actual public health goals. It was both useless and terrible.
So the news in last year's new National Drug Policy that a new Drug Harm Index would be developed from scratch and tied more obviously to the policy was very welcome.
The New Zealand Drug Harm Index 2016 was published yesterday. And it's ... better. Whether it's actually good is another matter.
Unlike the British DHI it cites, it does not include alcohol and tobacco, which clearly limits its application in policy assessment. And unlike the British DHI, it comes without clear targets in drug harm reduction.
But the author, Michael McFadden, has quite nicely dispensed with the "long tradition of including ‘intervention costs’ as harms" and does a good job of explaining why the cost of intervention (eg: policing) is an attempt to address harms and should not be considered a harm in itself.
This insert illustrates the potential dangers of including intervention costs as a type of harm. It is, of course, hypothetical.
Previous research has established that the sedative drug Stupor costs the community
$10 million annually in personal and community harms. No attempts have been made to address the growing threat from Stupor to date. An innovative and ongoing programme is introduced that reduces the harms associated with the sedative drug by 50%. The annual cost of the programme is $2.5 million. Under the traditional approach, the total harm associated with the drug is now $12.5 million and the return on investment is $2.50 for every dollar invested in the programme. In reality, the actual harm avoided remains at $10 million and the return on investment 2:1. The traditional method overestimates the benefits associated with an intervention when it includes those costs as part of the harm incurred.
This is good, and the introduction of foregone tax revenue on illicit drug commerce – which could be seen as a cost of prohibition – is interesting too. But elsewhere there are some obvious problems, such as the repeated conflation of natural cannabis and synthetic cannabinoids into one group as "cannabinoids". It really does not make sense to consider the two together when the harms associated with each are so unequal.
Moreover, it tends to jibe with another component of the index, the expert opinion survey. This survey is similar to one conducted in Scotland in 2011, but includes responses from far fewer experts. The Scottish survey had 290 respondents and McFadden approached 25 – of whom one declined to participate and 12 did not respond.
Disclosure: I was one of the 25 approached and one of the 12 non-responders. I did scrutinise the survey several times, but eventually didn't feel I could usefully respond to its requirement to score each drug 1-5 in terms of its "Personal Harms" and "Community Harms" for dependent and casual users respectively. Perhaps I should have tried harder, but it seemed a blunt instrument.
Nonetheless, the survey results are interesting:
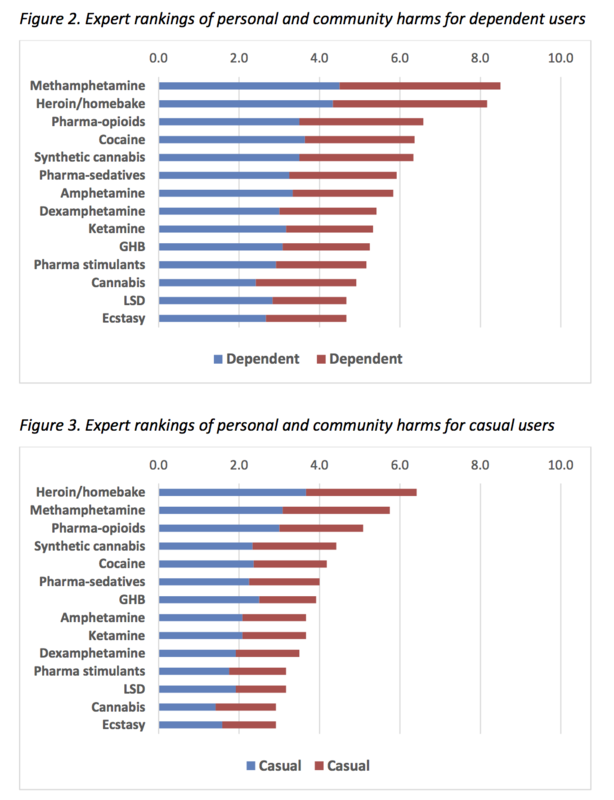
Cannabis (Class B or C, depending on form), LSD (Class A) and MDMA (Class B1) are rated as causing the lowest harms amongst both dependent and casual users, suggesting that our drug classfications need some bringing into order. But elsewhere in the survey – through the unwise combination of natural and synthetic cannabinoids, and the multiplication by number of users – total harms from cannabis are considered nearly equivalent to those of methamphetamine.
There are other questions about methodology, assumptions and presentation of data that are beyond my competence. I warmly invite the Public Address nerd crew to explore the index further.
For now, even McFadden emphasises that some of his methods are "innovative" and that the DHI is a "living document" that will be subject to change. In that respect, Minister Dunne might be best advised to greet it as a first step, rather than trumpeting it the way Jim Anderton did in 2008. Because as we know, that 2008 index did not match its billing.